A Question of Centimeters – Navigating the Tricky Waters of Surveillance and Watchful Waiting
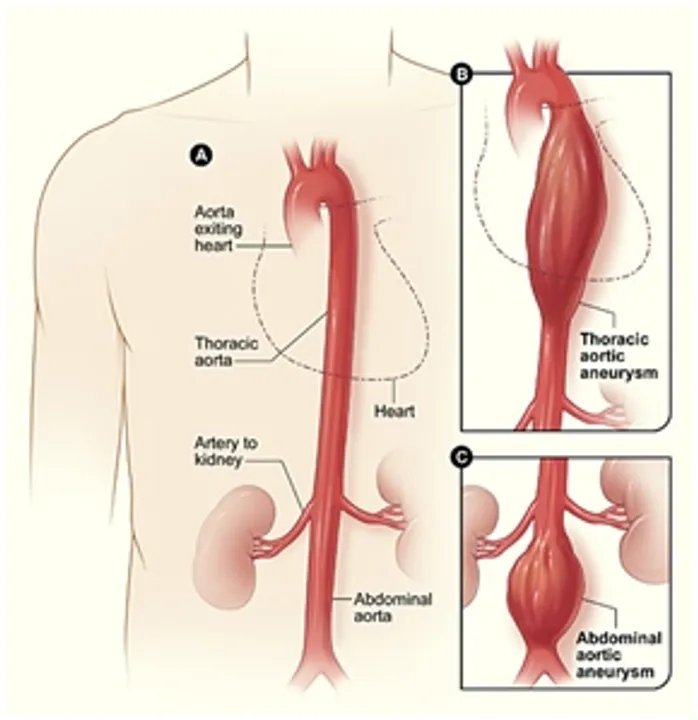
Image via cdc.gov
How long do you wait for a centimeter?
Let’s back up.
We already know the aorta is the major arterial vessel supplying oxygenated blood to the body. We understand that an aneurysm is a muscular weakening of any blood vessel wall that causes dilatation. When an abdominal aortic aneurysm (AAA) gets large enough, we worry that it will rupture, and the patient will die from decompensated shock.
What’s our cutoff? When is an abdominal aortic aneurysm too big? For the “average 70 kg male” that our medical journals insist on referencing (I’m 5’1” tall so excuse my bitterness), the aortic diameter measures 2.0 cm. When the diameter is greater than 150% of its normal size—i.e., greater than 3.0 cm—it’s officially an aortic aneurysm.
When do we operate? When do we decide enough is enough and surgically intervene to reduce the size of the AAA? Most vascular surgery centers establish a window of 5.0-5.5 cm aortic diameter before they decide to cut.
How would we even know to look for the aortic aneurysm in the first place? They don’t exactly elicit symptoms in patients, unless you count the severe flank pain and hematuria that occurs moments before they die. Otherwise, it’s a pretty silent problem. Instead, we find out about aortic aneurysms by screening the right population with a one-time abdominal ultrasound. According to the U.S. Preventative Services Task Force (USPSTF – rolls right off the tongue), that “right population” includes male smokers aged 65 to 75 years old (B Recommendation). If you’re a man who’s never smoked, physicians will be more selective about screening you with an ultrasound, and only a few will be checked (C Recommendation). If you’re a woman aged 65 to 75 who has smoked, there is insufficient evidence for routinely screening for AAAs (I Recommendation), and if you’re a woman who has never smoked, you’re not supposed to be screened at all (D Recommendation) – as in, the risks of screening for AAA in this population outweigh the benefits, so you shouldn’t do it.
Of course, my patient Mrs. D didn’t know any of this. Mrs. D is a 73-year-old divorced grandmother from Dunsville, Virginia who had never smoked a cigarette in her life. Rather, she said her vice was savory pies—think chicken pot pie, turkey pot pie, shepherd’s pie—both the construction and consumption thereof. Neither she, nor the dull epigastric pain she’d experienced for months, were aware that the USPSTF considered her aortic screening a “D Recommendation.” But when Mrs. D had an abdominal CT scan to explore her bowel discomfort, the radiologist couldn’t find a cause and incidentally found an abdominal aortic aneurysm, 4.6 cm in size.
Mrs. D was confused as to why this happened. I told her we don’t know exactly what causes AAAs, but that the two biggest risk factors were smoking tobacco and high cholesterol. She repeated that she’s never smoked in her life, before silently considering whether her pies were doing her in. I promised her this wasn’t the case: her cholesterol numbers were pretty good, and I’m not going to be the one who impugns pies.
So, what do we do now? The two most unwelcome words in primary care: watchful waiting.
The surveillance interval guidelines for AAAs are murky at best, and vary wildly by organization and country. In the U.S., consensus recommendations (for the epidemiologists keeping score, that is SOR C level assuredness) dictate that we can wait one year for any abdominal aortic aneurysms measuring 4.5 to 5.4 cm before performing a repeat surveillance abdominal CT scan.
There were a few problems with waiting a year for a scan, beyond Mrs. D worrying that this thing would blow up inside her. She wouldn’t be around this part of Virginia next March. Mrs. D would be living for a few months with her sister in Prince George, Virginia, and couldn’t drive the 1 hour and 15 minutes to the Tappahannock imaging center because her car recently died on Route 17 (her engine’s water pump failed while she was delivering a rabbit pie to an old high school friend). Mrs. D also knows that her sister uses her own car for work, and there are no public transportation options between the two counties. It doesn’t help that the only imaging center where most of the CT scan costs will be covered under Medicare is, again, in Tappahannock.
These reasons seemed much more valid to me than a consensus guideline to scan Mrs. D’s AAA in 1 year. So, to our original question:
How long do you wait for a centimeter?
In this case, we waited just 6 months. Not because of conflicting abdominal aortic aneurysm data, but to assuage a woman’s very reasonable fears. And to make sure she could get the imaging study done at a feasible cost -- and because of broken water pumps and rabbit pies.
References:
Related Posts
